The Life Skills Assessment Scale: Norms for young people aged 17–19 and 20–22 years
Main Article Content
Severe poverty, adversity, and malnutrition have irrefutable negative effects on the development and mental health of children and young people. The Life Skills Assessment Scale (LSAS), is a 5-item impact assessment scale developed in India, that provides a simple, yet valid and reliable, instrument to assess life skills of disadvantaged children and young people, with age norms of 8–16 years. In the present study, in Bengaluru, India, we used observational data obtained from 656 disadvantaged young people to extend the LSAS age norms to 17–19 and 20–22 years age groups, resulting in a simple, valid, and reliable assessment tool for children and young people aged from 8 to 22 years.
The global levels of extreme child poverty are not precisely known, as there is no standard definition of poverty nor is there a consistent approach to the collection of data. However, available figures show that, globally, from approximately 40% to 47% of children live with the effects of extreme poverty, surviving on less than US$2 per day: This percentage equates to hundreds of millions of children, of whom 30% are in India (Olinto, Beegle, Sobrado, & Uematsu, 2013; United Nations International Children’s Emergency Fund/World Bank, 2016; World Bank, 2018) where the current study took place. A key indication of extreme poverty is failure to thrive, commonly observed as stunted growth. Failure to thrive is associated with a wide range of long-term mental health and developmental issues. For example, it was estimated in the HUNGaMa Survey Report (Naandi Foundation, 2011) that in India the growth of up to 59% of all children under 5 years of age was stunted. Further, it was stated in the Indian government’s Children in India 2012 Statistical Appraisal (Ministry of Statistics and Programme Implication, 2012) that 48% of children in India under 5 years of age were affected by this condition. More recently, it was reported in the National Family Health Survey-4 in India (NFHS-4; International Institute for Population Sciences, 2017) that the 2015/2016 survey figures recorded that the growth of 38% of children under 5 years of age was stunted. NFHS-4 also stated that this rapid decline over the last decade appears to have stalled. However, globally both the World Bank (2018) and Geoghegan (2017) in a report for the Save the Children organization have stated that the number of children experiencing severe adversity is increasing as they are living in conflict areas and as members of displaced populations.
It is important to recognize that failure to thrive can happen in all stages of development and is associated with long-term or lifelong effects (Homan, 2016; Martorell, Rivera, Kaplowitz, & Pollitt, 1992). Stunted growth at 5 years of age will generally lead to problems in later development. Research examples include findings that stunted growth at 2 years of age can be linked to cognitive deficits at 9 years of age (Berkman, Lescano, Gilman, Lopez, & Black, 2002) and at 8 years and 11 years of age (Daniels & Adair, 2004; Mendez & Adair, 1999). Hoddinott et al. (2013) found in their longitudinal research that stunted growth at 72 months was associated with cognitive deficits in people aged from 25 to 42 years. Even if failure to thrive is completely remediated at a young age, the effects can continue for a generation as those 5-year-olds develop into adulthood. Although failure to thrive mostly comes about because of poor nutrition, even if adequate nutrition is available, adversity can also cause failure to thrive. Severe adversity for a child can involve being a refugee, living in a war zone, being abandoned, receiving institutional care, or having poor care arrangements.
Thousands of nongovernmental organizations (NGOs) provide interventions designed to ameliorate the negative effects of severe adversity, ranging from large multinational organizations to small local shelters caring for a handful of children or young people. Interventions to address malnutrition include supplementary feeding, and health- and social-improvement programs. Common life-skills interventions to address developmental and psychological needs include the teaching of life skills, programs in sports, creative arts, computer skills, and language skills, provision of camps, and mentoring. These interventions are designed to enhance development by facilitating young people’s ability to interact with others, by building up their skills, and enabling them to recognize and manage their emotions. A workable way to measure the outcome of interventions has been problematic. Although the physical measurement of weight and height is straightforward, it is much more difficult to measure developmental or psychological change. Staff in most NGOs use nonstandardized common sense measures (e.g., how many times does a young person attend programs or go to school), personal judgments, or just assume that interventions have worked. The Life Skills Assessment Scale (LSAS) is a simple, reliable, and valid measure of life skills interventions, which is currently in use in numerous developing countries (Kennedy, Pearson, Brett-Taylor, & Talreja, 2014). This study took place in India, but as the LSAS construction was based on child and adolescent development, it is culture and intervention generalizable. The LSAS does not assess any given activity but uses the notion of age-appropriate behavior in any activity or situation. As the LSAS is development-centered and culture and intervention free, it is generalizable to disadvantaged children and young people in developing countries outside India. NGO staff and facilitators have reported that young people aged up to about 22 years are using the programs, but the LSAS only had norms for those up to 16 years, so standardized assessments were not possible. Thus, in the current study we have added norms for the 17–19 and 20–22 years age groups.
Effects of Severe Childhood Adversity and Failure to Thrive
The terms extreme adversity, extreme poverty, and failure to thrive can be confusing. Extreme adversity can be experienced in many ways, and extreme poverty is an example of extreme adversity and can also cause failure to thrive or stunted growth. The probability of malnutrition being experienced by children and young people living in severe poverty is, of course, very high.
Failure to thrive is defined as a child not growing at a predetermined rate as measured by a growth chart. Growth charts cover development from birth to approximately 20 years of age (Centers for Disease Control and Prevention, 2000). Normally, children and young people grow in a set pattern, and growth charts are used to plot individual height, weight, and head circumference against a set standard. Stunted growth is used as a key indicator of failure to thrive as it is apparent and easy to measure using a standardized growth chart. Many disadvantaged children’s and young people’s growth patterns are abnormal in that they show changes in, or deviations from, the expected patterns of growth shown on the chart (e.g., below the 3rd or 5th percentile on a growth chart or crossing major percentiles), and these changes and/or deviations generally indicate failure to thrive. Although organic failure to thrive is most often caused by malnutrition (Homan, 2016), nonorganic failure to thrive can be caused by a range of severe adverse experiences.
Nonorganic failure to thrive is defined as a failure of growth with no organic reason, for example, abandonment, trauma, or abuse. However, the damaging effects of failure to thrive on development are the same whether the cause of the failure is organic or nonorganic. The effects of experiencing severe adversity and failure to thrive have been recognized for over a century (Holt, 1897) and have been irrefutably linked to attachment disorders, cognitive impairment, emotional and behavioral issues, neuropsychological abnormalities, and diagnoses of physical and mental-health disorders (see examples in Table 1). In the 1960s, failure to thrive was linked to a reactive attachment disorder that is included in the fifth edition of the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders (2013), which reflected its connection with developmental delay and mental health problems (Schwartz, 2000). Depending on the prevailing culture in which such issues occur, they may be described as symptoms of disorder or illness or as life-skills problems. The description/diagnosis may also depend on the services available in that location, that society’s perceptions, and the strength of the medical model. We conducted the current study in India where these issues are perceived as life-skills problems.
As cognitive impairment (see Table 1) describes an impact on areas such as children’s attention, memory, and information processing, it becomes very difficult, if not impossible, for children or young people whose growth is stunted or who have failed to thrive to reach individual capacity in learning, education, or vocational skills. United Nations International Children’s Emergency Fund (2009) described this situation as one of diminished learning capacity and poor school performance and Geoghegan (2017) of Save the Children described it as a lifetime of lost opportunities in education. Attachment disorder difficulties are associated with individuals being unable to tolerate closeness, attaching quickly to possibly inappropriate others, being unable to assert themselves, and experiencing emotion regulation difficulties, such as, being highly sensitive/insensitive to stress, lacking the ability to self-soothe and calm, and experiencing extreme inappropriate emotions. High anxiety levels may be interpreted as aggression, social withdrawal, avoidance, and absconding. At best, these issues make it difficult for the child or young person to thrive in the context of 21st century demands and, at worst, they establish the key foundations of future mental health issues.
Table 1. Examples of the Effects of Severe Childhood Adversity and Failure to Thrive
Life Skills Assessment Scale
A simple, valid, reliable, and accessible assessment instrument is needed for staff in NGOs to use to determine if their programs are effective in combating the effects of adversity. The LSAS 8–16 is currently in use in developing countries. However, NGO personnel have recognized that young people stay in programs and need care and support beyond 16 years of age, as they attempt to thrive. Thus, our aim was to construct norms of 17–19 and 20–22 years age groups.
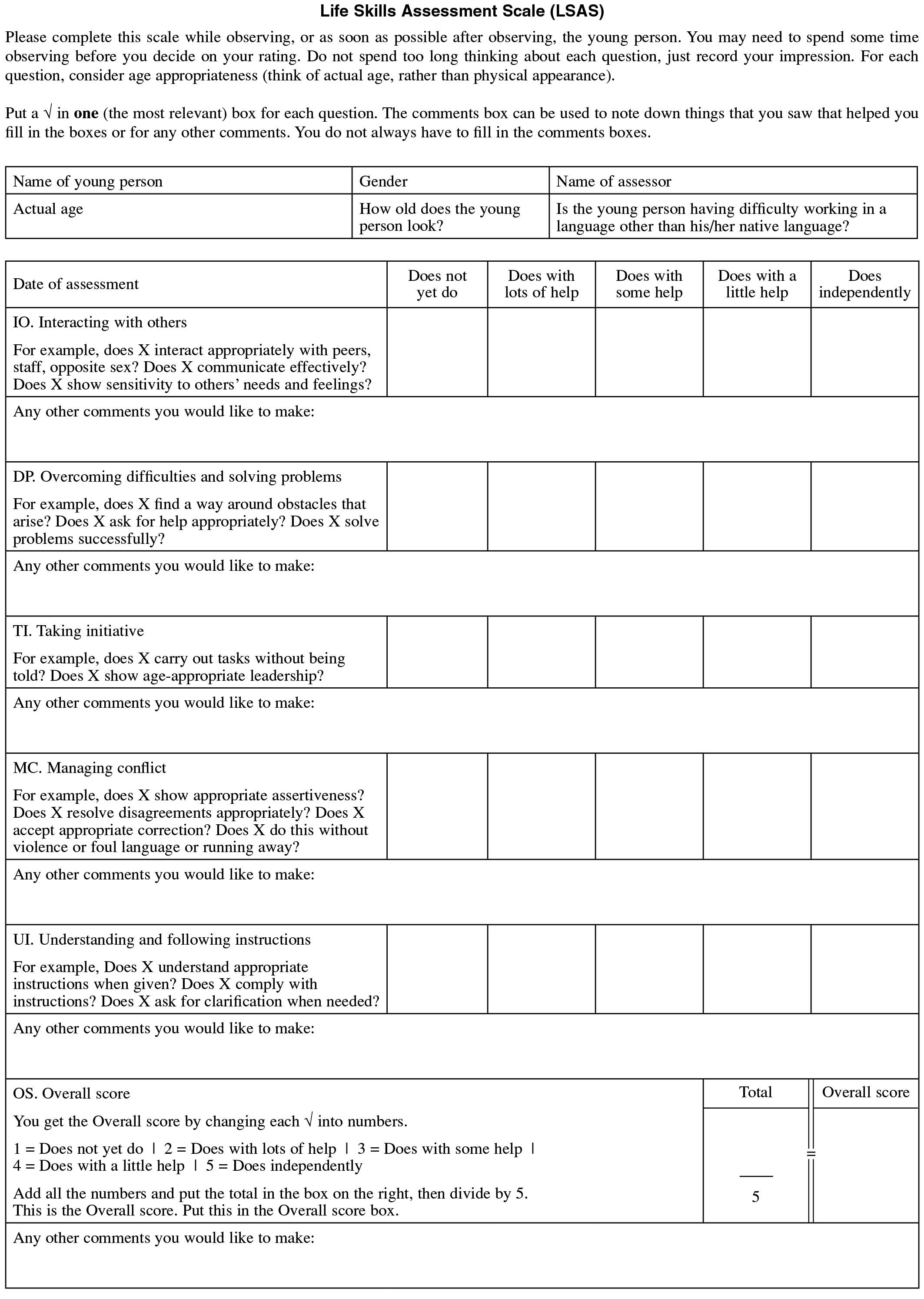
The LSAS is a five item, 5-point impact scale based on the World Health Organization’s (1997) definition of life skills (see Kennedy et al., 2014 for a full description) as follows: “Psychosocial competence is a person’s ability to deal effectively with the demands and challenges of everyday life. It is a person’s ability to maintain a state of mental well-being and to demonstrate this in adaptive positive behavior while interacting with others, his/her culture and environment.” The five life skills that the LSAS is designed to assess are: interacting with others, overcoming difficulties and solving problems, taking initiative, managing conflict, and understanding and following instructions.
Data based on observers’ responses to items concerning these five simple skills can provide a wide range of information, in a similar way to children’s developmental milestone assessments. They should not be seen as five discrete assessments but rather as indicators of areas of competence. For example, an observer can carry out a simple milestone assessment by asking a child to build a column of four play bricks. This is not intended as an assessment of the child’s play-brick-column-building ability but rather to enable the observer to assess the child’s fine motor skills and perception. The LSAS statements are often described as tips of the iceberg indicating broader areas of competence. Each item (dimension) is assessed on a 5-point Likert scale: 1 = does not yet do, 2 = does with lots of help, 3 = does with some help, 4 = does with a little help, 5 = does independently. Numbers can be attached to the Likert points, as shown above, for processing. However, when a simple scoring sheet is used, or when young people are assessed, we found it more effective not to have the numbers on the sheet as this could create an examination or pass/fail perception (see Appendix). As the LSAS was based on child and adolescent development together with age-appropriate life skills, it is culture and program free.
Uses of the Life Skills Assessment Scale
The LSAS has multiple uses depending on the type of assessment that is required by the user. It can be used to assess individual children, groups of children, and overall performance of programs or interventions. This means that the most effective programs can be identified and offered to individuals or groups of children and young people.
Individual young person assessment. An individual’s score can be compared to a normative score to ascertain if she or he is functioning in line with the population norm, or below (one standard deviation or more below the mean), or doing well (one standard deviation or more above the mean) in comparison with young people of the same age.
Life skills profiles can be produced to assess current strengths and development needs, for example, a young person may be able to take the initiative without help, but may need a lot of help in managing conflict without becoming aggressive. The assessment can be used interactively as appropriate with that young person individually and/or with carers, parents, teachers, and NGO staff to provide a program or intervention designed specifically to improve that young person’s management of conflict without becoming aggressive.
The effects of life skills programs or interventions on an individual can be assessed using the LSAS. Individual scores at Time A can be compared with scores at Times B or C, to assess progress on one of the five skills individually or on overall life skills. These results can be used to provide empirical evidence of progress and the assessor can then congratulate the individual on that progress, and/or can be used to choose further interventions/programs to build on this achievement. Alternatively, reductions in scores at Times B or C can be used as alerts that the current program or intervention is not meeting the needs of the young person and the individual who is working with the young person needs to give further attention to program/intervention selection.
An assessment based on the LSAS can be simply completed with a pen or pencil and the scoring sheet (see Appendix). If computing facilities are available graph-type representations are easily produced. A sample graph for an individual young person is shown in Figure 1.
Groups of young people or population assessment. The assessment can be used in a similar way for groups of young people or for populations by combining scores as in the above description. Graph representations can also be produced.
Outcome assessment and program comparison. A program or intervention can be evaluated through a comparison of the progress of groups of young people over time to assess if their life skills have improved and if the program or intervention is effective or ineffective.
The effects of the different programs on individual life skills can be assessed. In this assessment, programs’ strengths are highlighted and this enables the assessor to offer the most effective program according to the needs of the young people. For example, a computer-skills program may encourage the young person’s development of the life skill of taking initiative and solving problems, but may not contribute to the development of conflict-management skills.
A comparison of available programs with each other is useful to assess which type of program is the most effective for an individual young person in development both of overall life skills and of each specific life skill. This may be particularly useful when programs are being set up and developed to ensure that individual needs are met.
Who can use the Life Skills Assessment Scale?
Because of the simplicity of the assessment procedure, it can be used at various levels by any person individually or by staff in organizations that provide interventions to disadvantaged young people. The data can provide feedback to the young people themselves, and to their families. Other stakeholders who benefit from feedback may include teachers, researchers, funding bodies, partner organizations, and policymaking bodies.
Impact of a Program on an Individual Young Person
The progress of Saanvi, who lived in institutional care is shown in Figure 1, at the time of entry into the program (Time 1) and after attendance at daily evening sessions (Time 2). At Time 1, Saanvi scored poorly for overall life skills compared with her peer group. After 6 weeks (Time 2), Saanvi showed an overall significant increase in the score for life skills (1.4–2.6). However, Saanvi’s life-skill in interaction with others had not changed, according to the LSAS. The staff member working with Saanvi arranged for her to attend a program that had been shown by increases in the score for this skill in the LSAS to be successful at improving the ability of the individual to interact with others. As similar graphs can be produced to illustrate the impact and efficacy of whole programs, this can be valuable when a decision is being made about which program(s) would meet specific needs of individuals or groups of young people.
Figure 1. Preprogram and postprogram scores of Saanvi, a young woman.
Method
Ethical Considerations
All data collection took place during induction sessions that are a part of NGOs’ normal activities. Three of the observers/raters were paid an honorarium of Rs1,000 (approximately £10/US$12) per day to cover personal expenses.
Participants
Participants were 656 young people in two age groups 17, 18, and 19 years (n = 378) and 20, 21, and 22 years (n = 278), approximately equally gender divided (see Table 2). The makeup of the participant group was designed to reflect the general population of disadvantaged young people in India. Although the majority of participants were selected from an urban area, there was a mixture of rural and urban families, as rural families are rapidly migrating to formal (buildings) and informal (tents, temporary shelters) urban developments. Participants were from three groups: in formal education, not in a system, and in shelter care. Formal education is a wide description that includes preuniversity college through to part-time vocational training. Participants were in low cost or free courses, and came from poor socioeconomic areas, including slums. The term not in a system refers to young people who are not registered as being in education or formal employment, and includes young people who are street sellers, married and involved in family care, or informal laborers. The shelter-care group included young people who are in, or have recently left, shelter care, including orphanages, and those in conflict with the law. The figures in Table 2 are approximate as some participants may belong to more than one group, for example, they may be on a vocational course and living in a shelter or institution.
Table 2. Demographic Characteristics of the Young People
None of the young people had previously taken part in an NGO program designed to enrich or ameliorate the effects of adversity. Young people who opportunistically arrived at resource centers were recruited before the programs began, and were told to come back in a few days time when an induction session would be held before the programs started. The induction session was used to orientate the young person and collect data. At the resource centers programs are provided, such as reading and writing, and using a computer, and advice on vocational skills, money skills, and life skills, and the centers also serve as a safe place to be during the day where semistructured interactions take place. It is normal practice to have an orientation session before programs start to ensure that the young people’s needs will be met in the proposed programs and that they are participating in the most appropriate programs for their needs.
We also arranged for observers to go to education establishments, shelters, villages, and slum communities. We organized activities at which data could be gathered. The activities were a part of the normal work of the participating NGO and often formed the preprogram introduction. Observation of activities to check that programs meet the needs of the participating communities is usual practice for NGOs. Entry to programs was open to all participants.
Observers/Raters
There were 13 adult observers comprising six men and seven women, some of whom came from disadvantaged backgrounds themselves. They were all involved in NGO-type programs, but not at the centers being used for the research and not in that geographic area. Observers had no knowledge of the purpose of the study but were simply asked to observe an activity.
Procedure
We agreed on a standard activity based on the host NGO induction session in Bengaluru, India. We formed a steering group to establish the proportion of young people aged between 17 and 22 years needed to represent the population of disadvantaged young people (see Participants section). Young people living in shelter-type accommodation were offered a taster induction session that they could voluntarily join. During the observations, up to 20 young people took part in any one session. After the nonparticipant observers had assessed some sessions using the LSAS, they went to various locations where the sessions were organized. All available participants took part in the sessions and were assessed. The observers found that the young people did not generally exclude themselves from sessions. A pair of observers who did not communicate with each other collected interrater reliability data (two groups with 24 young people in each) during a session held at the same time for both groups. We also collected discriminant validity data during the induction sessions, with 24 disadvantaged young people and 24 advantaged young people from high-socioeconomic-level families in each of the two age groups. As it would not have been appropriate to offer the advantaged group an NGO induction-type session in the format used with disadvantaged young people, during these sessions the “advantaged” group took part in a football match. This activity was seen as acceptable, as football is a game that crosses cultures and societies, and thus no group had an advantage. We assessed reliability with a test and retest, with an interval of 14 days between the two tests.
Statistical Analysis
Participants in the validation study comprised 656 young people aged between 17 and 22 years (M = 18.93, SD = 1.64). As a visual inspection of histogram, boxplots, stem and leaf diagrams, and normality tests suggested nonnormal distribution of data, we used nonparametric statistics. We calculated the mean, standard deviation, and Cronbach’s alpha for the overall average scale score and for each item. Cronbach’s alpha with item deleted was used to test if each item made an individual contribution to the overall score. Mann-Whitney U and Wilcoxon W tests were used to test any differences between the two age groups of 17–19 years and 20–22 years. We also used the Mann-Whitney U test to assess gender differences within age groups. Finally, we calculated interrater and test-retest reliability using the F test and Wilks’ Δ to test differences, and to calculate discriminant validity.
Results
Descriptive Statistics for the Life Skills Assessment Scale
Descriptive statistics (mean and standard deviation) were produced for the overall score for the LSAS and for each LSAS item. The mean and standard deviation for the LSAS 8–16 years are included in Table 3 for comparison.
Table 3. Descriptive Statistics for the Life Skills Assessment Scale for 8–16 and 17–22 years
Note. LSAS = Life Skills Assessment Scale.
Data were analyzed to produce nonnormative scores (mean and standard deviation) for the two age groups (see Table 3). The Mann-Whitney U and Wilcoxon W tests showed a significant difference between age groups (z = -5.05, p < .001), with women (vs. men) scoring higher in the age group 17–19 years (p < .001). There were no gender differences in the 20–22 age group.
Reliability and Validity
The instrument showed excellent internal reliability (Cronbach’s α = .92), which was not improved by removing individual items. Thus, we considered that the overall score (average of the five subscales) could be used for remaining analyses. Interrater reliability was good (r = .76, p < .001) and test-retest reliability was excellent (r = .95, p < .001; Koo & Li, 2016). Regarding discriminative validity, a significant difference was found between the LSAS scores of the advantaged (vs. disadvantaged) groups (Δ = .18, p < .001), indicating that the LSAS (17–22 years) can discriminate between advantaged and disadvantaged young people.
Discussion
Statistical Properties of the Life Skills Assessment Scale
As descriptive statistics for the 17–19 and 20–22 age-group norms were similar to the norms for the 8-16 age group (see Table 3), the LSAS can be used seamlessly for practical everyday use with children and young people aged from 8 to 22 years. Results showed good reliability and validity of the scale.
Practical Considerations When the Life Skills Assessment Scale is Being Used
As the LSAS is observer rated, there is a need for some observer interpretation regarding age appropriateness and the amount of help needed to complete a task. As the statistical analysis indicated that observers are generally able to do this reliably, the scale can be used with confidence. We also found this to be the case for the original LSAS 8–16, which has now been used with disadvantaged children in many countries in the developing world. If desired, an explanatory session can be held or role-play scenarios acted out with new observers so that any questions about its administration can be raised. A free short web-based induction is available.
Use of Normative Data from the Life Skills Assessment Scale
In practical use, if a single life skill is being assessed, an individual score can change only in units of 1, owing to the scale structure. However, for multiple life skills assessments or assessment of multiple young people, the normative data of M = 2.7, SD = 0.74 can be used to make comparisons across time, groups, or programs. For example, a movement of 1.0 for an individual life skill would indicate a clear improvement or deterioration in the skill. For multiple life skills assessments or assessment of multiple young people (perhaps if overall efficacy of a program is being considered), we would consider a figure of 0.74 (approximately one standard deviation) as indicating a significant change. We recommend that when the LSAS is used for research, individual standard deviations are used to reliably assess precise change. The distribution of women’s scores in the 17–19 years group (vs. men) showed higher scores. Although the differences were modest and not relevant for practical use, this can be examined in future research.
Generalizability of the Life Skills Assessment Scale
Data for this study were gathered solely from disadvantaged young people in Bengaluru and surrounding areas in India. Although this is rapidly becoming an area with an urban population, because of economic migration locally and nationally, the young people came from a mixture of urban and rural backgrounds. We suggest that, as this scale is development-centered, it can be used worldwide with disadvantaged children or young people who are taking part in life-skills programs, as has been the case for the LSAS 8–16 years in various developing countries. All children negotiate the same developmental milestones and need an environment that enables them to do so. In all cultures, adversity and unmet basic needs result in similar developmental problems that can continue into adulthood (Hoddinott et al., 2013). However, as established life-skills assessment instruments (Nollan, Horn, Downs, Pecora, & Bressani, 2002) were developed for use in countries in the Western world, they are not designed to assess the impact of severe adversity, for example, severe poverty and malnutrition in developing countries. Although we cannot guarantee that the norms will be exactly the same in all developing countries, we expect them to be very similar. This has been confirmed by the use already made of the LSAS 8–16, as confirmed by the not-for-profit organization, HundrED, whose goal is to help improve education by encouraging pedagogically sound, ambitious innovations to spread across the world (HundrED.org, personal communication, November 9, 2019). Research is currently underway by the authors to establish confirmation of the accuracy of the age norms in other developing countries.
Summary
Our results showed that the LSAS is a simple, quick, yet reliable and valid instrument for use to measure life skills of disadvantaged young people in developing countries. These data can be added to the reliable and valid LSAS 8–16 to make a seamless assessment from 8–22 years. We believe that the LSAS is a unique standardized life skills measure for this age group.
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC: Author.
Benoit, D., & Coolbear, J. (2004). Disorders of attachment and failure to thrive. In L. Atkinson & S. Goldberg (Eds.), Attachment issues in psychopathology and intervention (pp. 49–64). London, UK: Erlbaum.
Berkman, D. S., Lescano, A. G., Gilman, R. H., Lopez, S. L., & Black, M. M. (2002). Effects of stunting, diarrhoeal disease, and parasitic infection during infancy on cognition in late childhood: A follow-up study. The Lancet, 359, 546–571.
https://doi.org/10.1016/S0140-6736(02)07744-9
Boddy, J., Skuse, D., & Andrews, B. (2000). The developmental sequelae of nonorganic failure to thrive. The Journal of Child Psychology and Psychiatry, 41, 1003–1014.
https://doi.org/10.1111/1469-7610.00688
Centers for Disease Control and Prevention. (2000). Growth charts. https://www.cdc.gov/growthcharts/
Daniels, M. C., & Adair, L. S. (2004). Growth in young Filipino children predicts schooling trajectories through high school. The Journal of Nutrition, 134, 1439–1446.
https://doi.org/10.1093/jn/134.6.1439
De Bellis, M. D., Spratt, E. G., & Hooper, S. R. (2011). Neurodevelopmental biology associated with childhood sexual abuse. Journal of Child Sexual Abuse, 20, 548–587.
https://doi.org/10.1080/10538712.2011.607753
Drewett, R. F., Corbett, S. S., & Wright, C. M. (2006). Physical and emotional development, appetite and body image in adolescents who failed to thrive as infants. The Journal of Child Psychology and Psychiatry, 47, 524–531.
https://doi.org/10.1111/j.1469-7610.2005.01529.x
Dykman, R. A., Casey, M. H., Ackerman, P. T., & McPherson, W. B. (2001). Behavioral and cognitive status in school-aged children with a history of failure to thrive during early childhood. Clinical Pediatrics, 40, 63–70.
https://doi.org/10.1177/000992280104000201
Essex, M. J., Klein, M. H., Cho, E., & Kalin, N. H. (2002). Maternal stress beginning in infancy may sensitize children to later stress exposure: Effects on cortisol and behavior. Biological Psychiatry, 52, 776–784.
https://doi.org/10.1016/S0006-3223(02)01553-6
Geoghegan, T. (2017). Stolen childhoods: End of childhood report 2017. London, UK: Save the Children.
Grantham-McGregor, S., Cheung, Y. B., Cueto, S., Glewwe, P., & Richter, L., & Strupp, B. (2007). Developmental potential in the first 5 years for children in developing countries. Lancet, 369, 60–70.
https://doi.org/10.1016/S0140-6736(07)60032-4
Hoddinott, J., Behrman, J. R., Maluccio, J. A., Melgar, P., Quisumbing, A. R., Ramirez-Zea, M., … Martorell, R. (2013). Adult consequences of growth failure in early childhood. The American Journal of Clinical Nutrition, 98, 1170–1178.
https://doi.org/10.3945/ajcn.113.064584
Holt, L. E. (1897). The diseases of infancy and childhood: For the use of students and practitioners of medicine. New York, NY: Appleton.
Homan, G. J. (2016). Failure to thrive: A practical guide. American Family Physician, 94, 295–299.
International Institute for Population Sciences, India. (2017). National Family Health Survey-4 (NFHS-4). Mumbai, India: Author.
Jaffe, A. C. (2011). Failure to thrive: Current clinical concepts. Pediatrics in Review, 32, 100–107.
https://doi.org/10.1542/pir.32-3-100
Kennedy, F., Kennerley, H., & Pearson, D. (Eds.). (2013). Cognitive behavioural approaches to the understanding and treatment of dissociation. London, UK: Routledge.
Kennedy, F., Pearson, D., Brett-Taylor, L., & Talreja, V. (2014). The Life Skills Assessment Scale: Measuring the life skills of disadvantaged children in the developing world. Social Behavior and Personality: An international journal, 42, 197–210.
https://doi.org/10.2224/sbp.2014.42.2.197
Kessler, R. C., McLaughlin, K. A., Green, J. G., Gruber, M. J., & Sampson, M. A., Zaslavsk, A. H., ... Williams, D. R. (2010). Childhood adversities and adult psychopathology in the WHO World Mental Health Surveys. The British Journal of Psychiatry, 197, 378–385.
https://doi.org/10.1192/bjp.bp.110.080499
Kinderman P., Schwannauer, M., Pontin, E., & Tai, S. (2013). Psychological processes mediate the impact of familial risk, social circumstances and life events on mental health. PLoS ONE, 8, e76564.
https://doi.org/10.1371/journal.pone.0076564
Koo, T. K., & Li, M. Y. (2016). A guideline of selecting and reporting intraclass correlation coefficients for reliability research. Journal of Chiropractic Medicine, 15, 155–163.
https://doi.org/10.1016/j.jcm.2016.02.012
Korzekwa, M. I., Dell, P. F., & Pain, C. (2009). Dissociation and borderline personality disorder: An update for clinicians. Current Psychiatry Reports, 11, 82–88.
https://doi.org/10.1007/s11920-009-0013-1
Larson-Nath, C., & Biank, V. F. (2016). Clinical review of failure to thrive in pediatric patients. Pediatric Annals, 45, e46–e49.
https://doi.org/10.3928/00904481-20160114-01
Mackner, L. M., Starr, R. H., Jr., & Black, M. M. (1997). The cumulative effect of neglect and failure to thrive on cognitive functioning. Child Abuse & Neglect, 21, 691–700.
https://doi.org/10.1016/S0145-2134(97)00029-X
Martorell, R., Rivera, J., Kaplowitz, J., & Pollitt, E. (1992). Long term consequences of growth retardation during early childhood. In M. Hernandez & J. Argenta (Eds.), Human growth: Basic and clinical aspects (pp. 143–149). Amsterdam, The Netherlands: Elsevier.
Mendez, M. A., & Adair, L. S. (1999). Severity and timing of stunting in the first two years of life affect performance on cognitive tests in late childhood. The Journal of Nutrition, 129, 1555–1562.
https://doi.org/10.1093/jn/129.8.1555
Ministry of Statistics and Programme Implementation, India. (2012). Children in India 2012: A statistical appraisal. New Delhi, India: Author.
Naandi Foundation. (2011). HUNGaMA: Fighting hunger and malnutrition: The HUNGaMA Survey Report 2011. Hyderabad, India: Author.
Nollan, K. A., Horn, M., Downs, A. C., Pecora, P. J., & Bressani, R. V. (2002). Ansell-Casey Life Skills Assessment (ACLSA) and life skills guidebook manual. Seattle, WA: Casey Family Programs.
Olinto, P., Beegle, K., Sobrado, C., & Uematsu, H. (2013). The state of the poor: Where are the poor, where is extreme poverty harder to end, and what is the current profile of the world's poor? World Bank-Economic Premise, 125, 1–8.
Pearson, D. (2013). Can the roots of dissociation be found in childhood? In F. Kennedy, H. Kennerley, & D. Pearson (Eds.), Cognitive behavioural approaches to the understanding and treatment of dissociation (pp. 40–52). London, UK: Routledge.
Read, J., & Bentall, R. P. (2012). Negative childhood experiences and mental health: Theoretical, clinical and primary prevention implications. The British Journal of Psychiatry, 200, 89–91.
https://doi.org/10.1192/bjp.bp.111.096727
Schwartz, I. D. (2000). Failure to thrive: An old nemesis in the new millennium. Pediatrics in Review. 21, 257–264.
https://doi.org/10.1542/pir.21-8-257
United Nations International Children’s Emergency Fund. (2009). The state of the world's children 2009: Maternal and newborn health. New York, NY: UNICEF.
United Nations International Children’s Emergency Fund/World Bank. (2016). Ending extreme poverty: A focus on children. Retrieved from https://uni.cf/2R7C5PM
van der Vegt, E. J. M., van der Ende, J., Huizink, A. C., Verhulst, F. C., & Tiemeier, H. (2010). Childhood adversity modifies the relationship between anxiety disorders and cortisol secretion. Biological Psychiatry, 68, 1048–1054.
https://doi.org/10.1016/j.biopsych.2010.07.027
World Bank. (2018). Poverty and shared prosperity 2018: Piecing together the poverty puzzle. Washington, DC: Author.
World Health Organization. (1997). Life skills education for children and adolescents in schools: Introduction and guidelines to facilitate the development and implementation of life skills programmes. Geneva, Switzerland: Author.
Appendix
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC: Author.
Benoit, D., & Coolbear, J. (2004). Disorders of attachment and failure to thrive. In L. Atkinson & S. Goldberg (Eds.), Attachment issues in psychopathology and intervention (pp. 49–64). London, UK: Erlbaum.
Berkman, D. S., Lescano, A. G., Gilman, R. H., Lopez, S. L., & Black, M. M. (2002). Effects of stunting, diarrhoeal disease, and parasitic infection during infancy on cognition in late childhood: A follow-up study. The Lancet, 359, 546–571.
https://doi.org/10.1016/S0140-6736(02)07744-9
Boddy, J., Skuse, D., & Andrews, B. (2000). The developmental sequelae of nonorganic failure to thrive. The Journal of Child Psychology and Psychiatry, 41, 1003–1014.
https://doi.org/10.1111/1469-7610.00688
Centers for Disease Control and Prevention. (2000). Growth charts. https://www.cdc.gov/growthcharts/
Daniels, M. C., & Adair, L. S. (2004). Growth in young Filipino children predicts schooling trajectories through high school. The Journal of Nutrition, 134, 1439–1446.
https://doi.org/10.1093/jn/134.6.1439
De Bellis, M. D., Spratt, E. G., & Hooper, S. R. (2011). Neurodevelopmental biology associated with childhood sexual abuse. Journal of Child Sexual Abuse, 20, 548–587.
https://doi.org/10.1080/10538712.2011.607753
Drewett, R. F., Corbett, S. S., & Wright, C. M. (2006). Physical and emotional development, appetite and body image in adolescents who failed to thrive as infants. The Journal of Child Psychology and Psychiatry, 47, 524–531.
https://doi.org/10.1111/j.1469-7610.2005.01529.x
Dykman, R. A., Casey, M. H., Ackerman, P. T., & McPherson, W. B. (2001). Behavioral and cognitive status in school-aged children with a history of failure to thrive during early childhood. Clinical Pediatrics, 40, 63–70.
https://doi.org/10.1177/000992280104000201
Essex, M. J., Klein, M. H., Cho, E., & Kalin, N. H. (2002). Maternal stress beginning in infancy may sensitize children to later stress exposure: Effects on cortisol and behavior. Biological Psychiatry, 52, 776–784.
https://doi.org/10.1016/S0006-3223(02)01553-6
Geoghegan, T. (2017). Stolen childhoods: End of childhood report 2017. London, UK: Save the Children.
Grantham-McGregor, S., Cheung, Y. B., Cueto, S., Glewwe, P., & Richter, L., & Strupp, B. (2007). Developmental potential in the first 5 years for children in developing countries. Lancet, 369, 60–70.
https://doi.org/10.1016/S0140-6736(07)60032-4
Hoddinott, J., Behrman, J. R., Maluccio, J. A., Melgar, P., Quisumbing, A. R., Ramirez-Zea, M., … Martorell, R. (2013). Adult consequences of growth failure in early childhood. The American Journal of Clinical Nutrition, 98, 1170–1178.
https://doi.org/10.3945/ajcn.113.064584
Holt, L. E. (1897). The diseases of infancy and childhood: For the use of students and practitioners of medicine. New York, NY: Appleton.
Homan, G. J. (2016). Failure to thrive: A practical guide. American Family Physician, 94, 295–299.
International Institute for Population Sciences, India. (2017). National Family Health Survey-4 (NFHS-4). Mumbai, India: Author.
Jaffe, A. C. (2011). Failure to thrive: Current clinical concepts. Pediatrics in Review, 32, 100–107.
https://doi.org/10.1542/pir.32-3-100
Kennedy, F., Kennerley, H., & Pearson, D. (Eds.). (2013). Cognitive behavioural approaches to the understanding and treatment of dissociation. London, UK: Routledge.
Kennedy, F., Pearson, D., Brett-Taylor, L., & Talreja, V. (2014). The Life Skills Assessment Scale: Measuring the life skills of disadvantaged children in the developing world. Social Behavior and Personality: An international journal, 42, 197–210.
https://doi.org/10.2224/sbp.2014.42.2.197
Kessler, R. C., McLaughlin, K. A., Green, J. G., Gruber, M. J., & Sampson, M. A., Zaslavsk, A. H., ... Williams, D. R. (2010). Childhood adversities and adult psychopathology in the WHO World Mental Health Surveys. The British Journal of Psychiatry, 197, 378–385.
https://doi.org/10.1192/bjp.bp.110.080499
Kinderman P., Schwannauer, M., Pontin, E., & Tai, S. (2013). Psychological processes mediate the impact of familial risk, social circumstances and life events on mental health. PLoS ONE, 8, e76564.
https://doi.org/10.1371/journal.pone.0076564
Koo, T. K., & Li, M. Y. (2016). A guideline of selecting and reporting intraclass correlation coefficients for reliability research. Journal of Chiropractic Medicine, 15, 155–163.
https://doi.org/10.1016/j.jcm.2016.02.012
Korzekwa, M. I., Dell, P. F., & Pain, C. (2009). Dissociation and borderline personality disorder: An update for clinicians. Current Psychiatry Reports, 11, 82–88.
https://doi.org/10.1007/s11920-009-0013-1
Larson-Nath, C., & Biank, V. F. (2016). Clinical review of failure to thrive in pediatric patients. Pediatric Annals, 45, e46–e49.
https://doi.org/10.3928/00904481-20160114-01
Mackner, L. M., Starr, R. H., Jr., & Black, M. M. (1997). The cumulative effect of neglect and failure to thrive on cognitive functioning. Child Abuse & Neglect, 21, 691–700.
https://doi.org/10.1016/S0145-2134(97)00029-X
Martorell, R., Rivera, J., Kaplowitz, J., & Pollitt, E. (1992). Long term consequences of growth retardation during early childhood. In M. Hernandez & J. Argenta (Eds.), Human growth: Basic and clinical aspects (pp. 143–149). Amsterdam, The Netherlands: Elsevier.
Mendez, M. A., & Adair, L. S. (1999). Severity and timing of stunting in the first two years of life affect performance on cognitive tests in late childhood. The Journal of Nutrition, 129, 1555–1562.
https://doi.org/10.1093/jn/129.8.1555
Ministry of Statistics and Programme Implementation, India. (2012). Children in India 2012: A statistical appraisal. New Delhi, India: Author.
Naandi Foundation. (2011). HUNGaMA: Fighting hunger and malnutrition: The HUNGaMA Survey Report 2011. Hyderabad, India: Author.
Nollan, K. A., Horn, M., Downs, A. C., Pecora, P. J., & Bressani, R. V. (2002). Ansell-Casey Life Skills Assessment (ACLSA) and life skills guidebook manual. Seattle, WA: Casey Family Programs.
Olinto, P., Beegle, K., Sobrado, C., & Uematsu, H. (2013). The state of the poor: Where are the poor, where is extreme poverty harder to end, and what is the current profile of the world's poor? World Bank-Economic Premise, 125, 1–8.
Pearson, D. (2013). Can the roots of dissociation be found in childhood? In F. Kennedy, H. Kennerley, & D. Pearson (Eds.), Cognitive behavioural approaches to the understanding and treatment of dissociation (pp. 40–52). London, UK: Routledge.
Read, J., & Bentall, R. P. (2012). Negative childhood experiences and mental health: Theoretical, clinical and primary prevention implications. The British Journal of Psychiatry, 200, 89–91.
https://doi.org/10.1192/bjp.bp.111.096727
Schwartz, I. D. (2000). Failure to thrive: An old nemesis in the new millennium. Pediatrics in Review. 21, 257–264.
https://doi.org/10.1542/pir.21-8-257
United Nations International Children’s Emergency Fund. (2009). The state of the world's children 2009: Maternal and newborn health. New York, NY: UNICEF.
United Nations International Children’s Emergency Fund/World Bank. (2016). Ending extreme poverty: A focus on children. Retrieved from https://uni.cf/2R7C5PM
van der Vegt, E. J. M., van der Ende, J., Huizink, A. C., Verhulst, F. C., & Tiemeier, H. (2010). Childhood adversity modifies the relationship between anxiety disorders and cortisol secretion. Biological Psychiatry, 68, 1048–1054.
https://doi.org/10.1016/j.biopsych.2010.07.027
World Bank. (2018). Poverty and shared prosperity 2018: Piecing together the poverty puzzle. Washington, DC: Author.
World Health Organization. (1997). Life skills education for children and adolescents in schools: Introduction and guidelines to facilitate the development and implementation of life skills programmes. Geneva, Switzerland: Author.
Table 1. Examples of the Effects of Severe Childhood Adversity and Failure to Thrive
Figure 1. Preprogram and postprogram scores of Saanvi, a young woman.
Table 2. Demographic Characteristics of the Young People
Table 3. Descriptive Statistics for the Life Skills Assessment Scale for 8–16 and 17–22 years
Note. LSAS = Life Skills Assessment Scale.
The authors acknowledge the tireless contributions of Kanthi Krishnamurthy
Annie Jacob
Khushboo Kumari
Sheetal Lydia Prasad
and Chandrasekhar.
No author has any financial or similar interest in connection with this study
and all authors contributed voluntarily. There was no specific funding for the study and there is no charge for the assessment sheet.
David Pearson, The Boulders, Quarr Road, Ryde PO33 4EL, UK. Email: [email protected]