Perceived stress, self-efficacy and its relations to psychological well-being status in Iranian male high school students
Main Article Content
Psychological stress has been found to be associated with a variety of ailments and health outcomes in adolescents. This study investigated the relationships between perceived stress, general self-efficacy and mental health status among Iranian male adolescents recruited from midtown high schools in Tehran who studied in 12th grade (N = 148). Pupils completed three questionnaires for assessing perceived stress (PSS-14; Cohen, Kamarck, & Mermelstein, 1983), general self-efficacy (GSE; Schwarzer & Jerusalem, 1995) and psychological well-being (GHQ-28; Goldberg & Hillier, 1979). Statistical analysis revealed that greater stress was associated with lower general self-efficacy and lower mental health status. A significant inverse relationship between self-efficacy and general health was found among these students. Results are discussed in relation to their implications for effective mental health education (e.g., stress management training) for adolescents.
During the past two decades, the construct of “stress” has received significant investigative attention as a correlate or predictor of psychological and health outcomes (Cohen, Kessler, & Gordon, 1995; Dougall & Baum, 2001). The causal mechanism by which stress affects the health of adolescents is not definitively known at present. However, a widely accepted view is that stressors result in changes in the autonomic nervous system, neuromuscular system, neurotransmitter integrity, endocrine and/or immunological functioning that increases the probability that an illness will develop (Brantley & Ames, 2001; Kiecolt- Glaser, McGuire, Robles, & Glaser, 2002).
In addition to the direct effects of physiological function that stressors may have, stressors may also have indirect effects on health. Specifically, increases in behavioral risk factors for illness such as increased use of alcohol, tobacco, or decreased sleep may accompany increased levels of stress (Cohen, Kessler, & Gordon, 1995). Moreover, psychological stress has been found to be associated with a variety of ailments and health outcomes in adolescents, including poor general physical health (Baldwin, Harris, & Chambliss, 1997), depressive symptoms (Unger et al., 2001), and smoking initiation, continued smoking, or relapse to smoking following smoking cessation treatment (Byrne & Mazanov, 2001; Wills, Sandy, & Yaeger, 2002).
One of the important factors that affects mental health status and appropriate responses to stressors is high self-efficacy. Some studies have reported the importance of self-efficacy on adolescents’ mental health (Muris, 2002; Muris, Schmidt, Lambrichs, & Meesters, 2001). Self-efficacy is a focal determinant because it affects health behavior, both directly and by its influence on the other determinants. Self-efficacy beliefs influence goals and aspiration. Self-efficacy beliefs shape the outcomes people expect their efforts to produce. Those of high self-efficacy expect to realize favorable outcomes. Conversely, those with low self-efficacy expect their efforts to result in poor outcomes (Bandura, 2004). Some studies support the moderating effect of self-efficacy and its influence on psychological well-being in relation to stressful experiences (Arnstein, Caudill, Mandle, Norris, & Beasley, 1999; O’Leary, 1992; Schiaffino & Revenson, 1992). Furthermore, Maciejewski, Prigerson, and Mazure (2000) have found relationships between stressful life events and overall mood disturbance.
Adolescence is a dynamic time in an individual’s life. While many changes during this time can be exciting and challenging, others can be extremely stressful. Importantly, some adolescents are bombarded with stressful events that they have little or no control over, especially those from underrepresented groups (Figueira-McDonough, 1998). Compounding this problem, adolescents may not have a well-developed coping repertoire because of limited life experiences, thus relying on only a handful of coping strategies to deal with stressors.
Adolescents comprise a significant part of today’s population: one in five people worldwide are adolescents between 10 and 19 years of age, and 85% of adolescents live in developing countries (Keeney, Cassata, & McElmury, 2004). In Iran there are 18 million young Iranians and 27.2% of the total population is between 10 to 19 years of age (IRIMHME, 2000).
Because of a lack of research about psychological well-being status and its relation to stress and self-efficacy among adolescence people in Iran, and in accordance with the above mentioned background, the purpose of the present study was to investigate the relationships between mental health status, perceived stress and general self-efficacy among Iranian male high school students.
Method
Participants and Procedure
This study was part of a large project conducted among male high school students in Tehran during the 2005-2006 school year, the main goal of which was to promote mental health among 12th grade high school students. The present study focused on assessing and analyzing the relationship between perceived stress, general self-efficacy and mental health status in adolescent students. After coordinating with high school managers and having obtained approval from the relevant university ethical committee and permission from the students’ parents, this project was carried out.
All subjects were selected from Tehran’s Number 6 district area, which included five high schools for male adolescents. Two high schools were chosen. The students who were studying at 12th grade level were selected from each high school. Based on randomized sampling allocation, from a total of 866 students, 154 students with an average age of 17.5 were recruited in this study.
Prior to conducting the main project, a pilot study was carried out. Initially the relevant questionnaires were administered to 31 adolescents who were similar to participants in the main study to obtain feedback about the clarity, length, comprehensiveness, time of completion, and also internal reliability (Cronbach’s alpha coefficient) of the measures. Before completing the questionnaires, participants were instructed about how to do this. After excluding incomplete questionnaires, the response rate for the main project was 94.3% (N = 148).
Measures
Demographics Background data were studied in this study such as: age, course of study (i.e., mathematics, natural sciences), birth rank, number of family members, parents’ educational status, household economic status based on reported parental income and economic indices for classification of income in Iran (i.e., good, moderate, bad).
Psychological well-being Psychological well-being was measured by the Persian version of Goldberg’s General Health Questionnaire (GHQ-28). The questionnaire containing 28 items was developed by Goldberg and Hillier (1979). The four subscales, each containing seven items are: A - somatic symptoms (items 1-7), B - anxiety/insomnia (items 8-14), C - social dysfunction (items 15-21), and D - severe depression (items 22-28). For identifying caseness with GHQ-28, the total of the subscales is used. The items are scored on a four point scale (0-3). A higher score indicates more distress and respondents who had a score of 23 or higher were identified as having psychological caseness (Goldberg & Williams, 1988; Goldberg et al., 1997). A reliability coefficient was calculated for GHQ-28 (α = 0.89). This result demonstrated that the GHQ-28 was internally consistent.
Perceived stress Subjective stress was assessed by the Cohen’s perceived stress scale (Cohen, Kamarck, & Mermelstein, 1983). The Persian translation of the perceived stress scale was used to assess the degree to which situations in life experienced during the previous month are perceived as stressful. The version used here had 14 items and the simple Likert method scoring (0 to 4) was applied. Higher scores on the scale indicated more levels of perceived stress. A reliability coefficient was calculated for the PSS-14 (α = 0.78). This result revealed that the Persian version of PSS-14 was internally consistent.
Self-efficacy In this study Schwarzer’s 10-item General Self-Efficacy Scale (GSE; Schwarzer & Jerusalem, 1995) was used. Nezami, Schwarzer, and Jerusalem (1996) translated the original scale (in German) into Persian. The GSE Scale was created to assess a general sense of perceived self-efficacy with the aim in mind to predict coping with daily hassles as well as adaptation after experiencing all kinds of stressful life events. Responses are made on a 4-point scale (1 to 4). Summing the responses to all 10 items yields the final composite score with a range from 10 to 40. Higher scores on the scale indicated more levels of perceived general self-efficacy. Reliability coefficients were calculated for the self-efficacy scale (α = 0.85) and demonstrate internal consistency.
Results
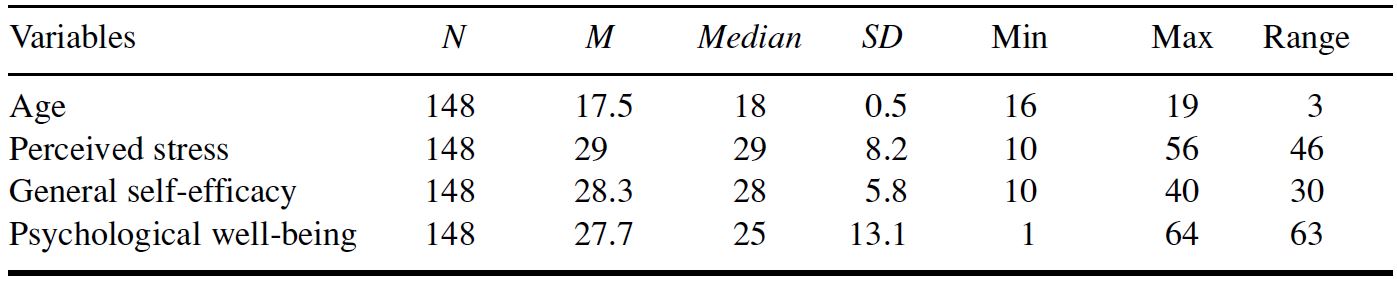
The purpose of this study was to examine whether or not there are relationships between high school male students’ perceived stress levels and psychological well-being and GSE status, also assessing associations between these variables with some demographic characteristics including age, economics, and course of study. Analyses were conducted by using SPSS 11.5 and a probability level of 0.05 was used throughout. A summary of descriptive statistics related to the distribution of the main variables was presented in Table 1.
Table 1. Descriptive Data for Age, Perceived Stress, General Self-Efficacy and Psychological Well-Being
Intercorrelations among the perceived stress, GSE and psychological well-being measures are presented in Table 2. As is apparent from Table 2, perceived stress displayed the most obvious stress-related influence on variance in stress-reported psychological disturbance. Negative relationships between perceived stress and psychological distress with GSE were observed. The positive correlation between perceived stress and psychological distress was statistically significant (r = 0.63, p < 0.01).
Table 2. Intercorrelation Among Measures of Perceived Stress, Self-Efficacy and Psychological Well-Being
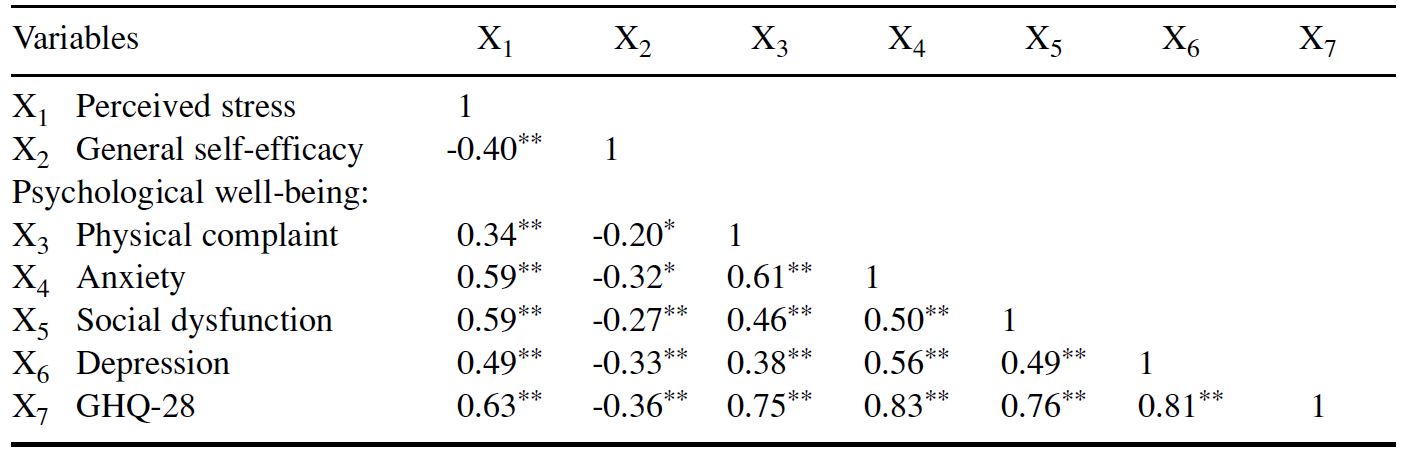
Notes: (N = 148) *p < 0.05, **p < 0.01
As mentioned before, psychological distress is measured by General Health Questionnaire (GHQ-28) and the threshold score in order to decide on probable levels of morbidity is 23. Therefore, respondents were divided to psychiatric caseness (58.8%, n = 87) and noncase (41.2%, n = 61). According to the median scores of GSE and perceived stress, we divided all subjects into low or high level of self-efficacy and perceived stress. Thus, low scorers were those who had perceived stress scores less than 29 (n = 66, 44.6%) and GSE score less than 28 (n = 62, 41.9%).
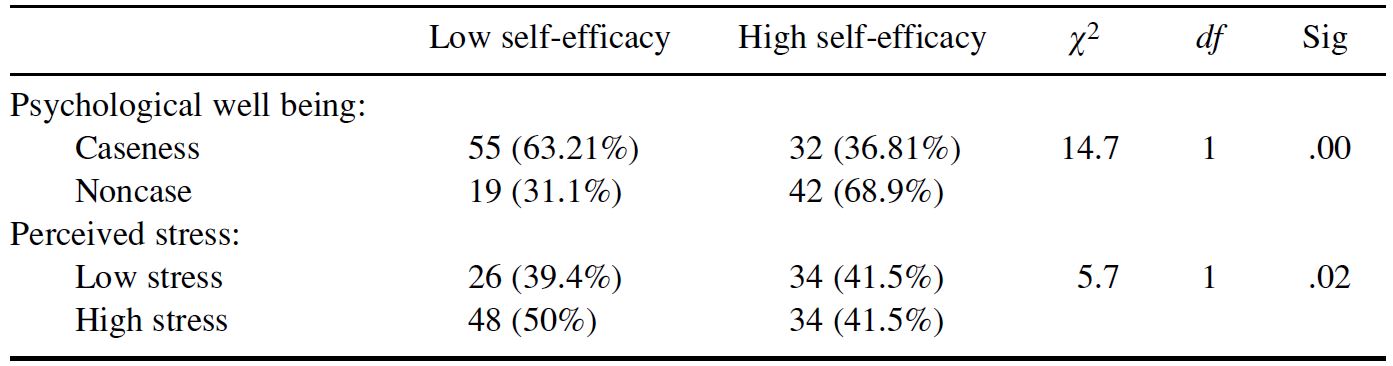
As is apparent from Table 1 and Table 2, perceived stress and psychological well-being scores increased as self-efficacy scores decreased. A chi-square test was used in the sample in order to assess the relationship between low self-efficacy and psychological status (caseness or noncase) and stress level (low or high). As Table 3 makes clear there is a significant relationship among students with low self-efficacy regarding to the psychological well-being and level of stress.
A chi-square test analysis revealed that there is no significant difference between students of mathematics and natural sciences for psychological problems (χ2 = 0.005, df = 0.1, p = 0.94). Findings also showed that there are significant relationships between low self-efficacy with existing psychological well-being and stress among students (Table 3).
Table 3. Comparing Students with High and Low Levels of Self-Efficacy in Relation to Perceived Stress and Psychological Well-Being
Multiple regression analyses indicated that perceived stress and self-efficacy significantly determined psychological well-being and the interaction obtained accounted for an additional 42% of the variance in psychological distress (multiple r = 0.64, p = .000). The perceived stress scores were a better predictor of total psychological well-being scores (β = 0.58, p = 0.000) than were the GSE scores (β = -0.12, p = 0.07).
A chi-square test was used in order to assess the relationship between levels of stress (low or high) and psychological well-being. Results showed that there is a significant relationship among students with high perceived stress regarding psychological caseness. In addition 80.5% (n = 66) with a high level of perceived stress have had psychological problems (χ2 = 35.7, df = 1, p = .000).
A zero-order correlation was applied for assessing associations between birth rank and number of household family and age of subjects with perceived stress, GSE and psychological well-being scores. A two-tailed test at significance levels of 0.05 was the criteria for the Pearson correlation between variables and analyses revealed that the relation between those variables showed no significance.
One-way ANOVA revealed that there were no significant relationships between perceived stress, GSE and psychological well-being scores based on parents’ educational status at p < 0.05. Regarding family status, chi-square tests showed that there were no significant relationships between participants living with both parents or one parent regarding the perceived stress, GSE and psychological well-being scores at significance levels of 0.05.
Discussion
The purpose of this study was to assess the perceived stress among male high school students and its relationship to self-efficacy and psychological well-being. Consistent with prior research, the findings of the current study indicate that there are significant relationships between self-efficacy, perceived stress and psychological well-being. High self-efficacy was related to increased psychological well-being status (Cheung & Sun, 2000; Endler, Kocovski, & Macrodimitris, 2001; O’Leary, 1992; Schiaffino & Revenson, 1992; Shelley & Pakenham, 2004). As mentioned in the results, interrelationships between stress and psychological distress were seen in this study and these are similar to other studies in the same context (e.g., Cohen et al., 1983; Rawson, Bloomer, & Kendall, 1994; Unger et al., 2001). What is clear is that the associations between perceived stress, self-efficacy and psychological well-being in this study were not mediated by differences in demographic characteristics.
Stress is not a new concept but the word itself has become extremely fashionable in the rapidly changing culture of the past few decades. However, stress is not always detrimental but could indeed be advantageous. Some individuals need a certain level of stress or eustress in order to enable them to function effectively (Monk, 2004). Selye’s (1956) research into stress indicated that each individual has an optimum level of stress, that is, what will cause stress for one person will merely result in eustress for another, enabling that individual to perform better than he/she would if levels of stress were lower. The past decade has seen the emergence of cognitive-behavioral treatment programs for children and adolescents with anxiety disorders and depression (Kendall, 1994; Lewinsohn, Clarke, Hops, & Andrews, 1990). There are strong indications that increasing self-efficacy should be considered as an important target of psychotherapy (Bandura, 1997).
Life events are stressors, which can interact with other variables to cause stress in students. Examinations, too, exert much pressure on students but this can be affected by such variables as personality, self-esteem and locus of control (Clarke, 1995; Monk, 2004). Our study provides the suggestion for assessing these variables in future studies in a similar context.
Although the present study has several strengths, such as being theory driven, having an adequate sample size, psychometrically sound measures, and a multidomain measure of psychological well-being, self-efficacy and stress, the study is limited due to the homogenous sample. Future studies in this context may also improve on the present study by sampling older and diverse populations, as similar studies have done (Pakenham, 1999; Schiaffino & Revenson, 1992).
It seems obvious that increased counseling facilities and stress management training programs with the inclusion of a specialist mental health facility for students are imperative. Stress management training cannot alter the inevitable, but it can help to make adolescents more aware, able to manage and cope better with stressful situations, receptive to change and accepting of what is unavoidable, restructuring of cognitions, etc. It is hoped that such studies will be extended to encompass all of the many adolescents in need.
References
Arnstein, P., Caudill, M., Mandle, C. L., Norris, A., & Beasley, R. (1999). Self-efficacy as a mediator of the relationship between pain intensity, disability and depression in chronic pain patients. Pain, 80, 483-491.
Baldwin, D. R., Harris, S. M., & Chambliss, L. N. (1997). Stress and illness in adolescence: Issues of race and gender. Adolescence, 32, 839-853.
Bandura, A. (1997). Self-efficacy: The exercise of control. New York: Freeman
Bandura, A. (2004). Health promotion by social cognitive means. Health Education & Behavior, 31 (2), 143-164.
Brantly, P. J., & Ames, S. C. (2001). Psychology of health and disease. In P. B. Sutker & H. E. Adams (Eds.), Comprehensive handbook of psychopathology (pp. 777-795). New York: Plenum.
Byrne, D. G., & Mazanov, J. (2001). Self-esteem, stress and cigarette smoking in adolescents. Stress and Health, 17, 105-110.
Cheung, S. K., & Sun, S. Y. K. (2000). Effect of self-efficacy conditions of mutual-aid organization members. Social Behavior and Personality: An international journal, 28 (5), 413-422.
Clarke, D. E. (1995). Vulnerability to stress as a function of age, sex, locus of control, hardiness and type A personality. Social Behavior and Personality: An international journal, 23 (3), 285-286.
Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24, 385-396.
Cohen, S., Kessler, R. C., & Gordon, L. U. (1995). Strategies for measuring stress in studies of psychiatric and physical disorders. In S. Cohen, R. C. Kessler, & L. U. Gordon (Eds.), Measuring stress: A guide for health and social scientists (pp. 80-101). New York: Oxford University Press.
Cohen, S., & Williamson, G. (1988). Perceived stress in a probability sample of the United States. In S. Spacapan & S. Oskamp (Eds.), The social psychology of health (pp. 31-67). Newbury Park, CA: Sage.
Dougall, A. L., & Baum, A. (2001). Stress, health and illness. In A. Baum, T. A. Reversion, & J. E. Singer (Eds.), Handbook of health psychology (pp. 321-337). Mahwah, NJ: Lawrence Erlbaum.
Endler, N. S., Kocovski, N. L., & Macrodimitris, S. D. (2001). Coping, efficacy, and perceived control in acute versus chronic illness. Personal and Individual Differences, 30, 617-625.
Figueria-McDonough, J. (1998). Voices of young people in poor inner-city neighborhoods. Youth and Society, 30, 123-163.
Goldberg, D. P., & Hillier, V. (1979). A scaled version of the General Health Questionnaire. Psychological Medicine, 9, 139-145.
Goldberg, D. P., & Williams, P. A. (1988). A user’s guide to the General Health Questionnaire. Berkshire, England: NFER-Nelson.
Islamic Republic of Iran, Ministry of Health and Medical Education (IRIMHME). (2000). Iran demographic and health survey /DHS-2000, p.9.
Keeney, G. B., Cassata, L., & McElmury, B. J. (2004). Adolescent health and development in nursing and midwifery education. Retrieved November 25, 2005, from http://www.who.int/child-adolescent-health/New-publication/aDH/WHO-FCH-CaH.
Kendall, P. C. (1994). Treating anxiety disorders in children: Results of a randomized clinical trial. Journal of Consulting and Clinical Psychology, 62, 100-110.
Kiecolt-Glaser, J. K., McGuire, L., Robles, T. F., & Glaser, R. (2002). Psychoneuroimmunology: Psychological influences on immune function and health. Journal of Consulting and Clinical Psychology, 70, 537-547.
Lewinsohn, P. M., Clarke, G. N., Hops, H., & Andrews, J. (1990). Cognitive-behavioral group treatment of depression in adolescents. Behavior Therapy, 21, 385-401.
Maciejewski, P. K., Prigerson, H. G., & Mazure, C. M. (2000). Self-efficacy as a moderator between stressful life events and depressive symptoms: Differences based on history of prior depression. British Journal of Psychiatry, 176, 373-378.
Monk, E. M. (2004). Student mental health: The case studies. Counseling Psychology Quarterly, 17 (4), 395-412.
Muris, P. (2002). Relationships between self-efficacy and symptom of anxiety disorders and depression in a normal adolescent sample. Personality and Individual Differences, 32 (2), 337- 348.
Muris, P., Schmidt, H., Lambrichs, R., & Meesters, C. (2001). Protective and vulnerability factors of depression in normal adolescents. Behavior Research and Therapy, 39 (5), 555-565.
Nezami, E., Schwarzer, R., & Jerusalem, M. (1996). Persian adaptation of the General Self-Efficacy Scale. Retrieved on November 15, 2004, from http://www.userpage.Fu-berlin.De/health /Persian. html
Pakenham, K. I. (1999). Adjustment to multiple sclerosis: Application of a stress and coping model. Health Psychology, 18, 383-392.
Rawson, H. E., Bloomer, K., & Kendall, A. (1994). Stress, anxiety, depression and physical illness in college students. Journal of Genetic Psychology, 155 (3), 321-33.
Schiaffino, K. M., & Revenson, T. A. (1992). The role of perceived self-efficacy, perceived control and causal attributions in adaptation to rheumatoid arthritis: Distinguishing mediator from moderator effects. Personality and Social Psychology Bulletin, 18, 709-718.
Schwarzer, R., & Jerusalem, M. (1995). Generalized Self-efficacy Scale. In J. Weinman, S. Wright, & M. Johnston (Eds.), Measures in health psychology: A user’s portfolio. Causal and control beliefs (pp. 35-37). Windsor, UK: NFER-Nelson.
Selye, H. (1956). The stress of life. New York: McGraw-Hill.
Shelley, M., & Pakenham, K. I. (2004). External health locus of control and general self-efficacy: Moderators of emotional distress among university students. Australian Journal of Psychology, 56 (3), 191-199.
Unger, J. B., Li, Y., Johnson, C. A., Gong, J., Chen, X., Li, C. V., Trinidad, D. R., Tran, N. T., & Lo, A. T. (2001). Stressful life events among adolescents in Wuhan, China: Association with smoking, alcohol use and depressive symptoms. International Journal of Behavioral Medicine, 8, 1-18.
Wills, T. A., Sandy, J. M., & Yaeger, A. M. (2002). Stress and smoking in adolescence: A test of directional hypotheses. Health Psychology, 21, 122-130.
Arnstein, P., Caudill, M., Mandle, C. L., Norris, A., & Beasley, R. (1999). Self-efficacy as a mediator of the relationship between pain intensity, disability and depression in chronic pain patients. Pain, 80, 483-491.
Baldwin, D. R., Harris, S. M., & Chambliss, L. N. (1997). Stress and illness in adolescence: Issues of race and gender. Adolescence, 32, 839-853.
Bandura, A. (1997). Self-efficacy: The exercise of control. New York: Freeman
Bandura, A. (2004). Health promotion by social cognitive means. Health Education & Behavior, 31 (2), 143-164.
Brantly, P. J., & Ames, S. C. (2001). Psychology of health and disease. In P. B. Sutker & H. E. Adams (Eds.), Comprehensive handbook of psychopathology (pp. 777-795). New York: Plenum.
Byrne, D. G., & Mazanov, J. (2001). Self-esteem, stress and cigarette smoking in adolescents. Stress and Health, 17, 105-110.
Cheung, S. K., & Sun, S. Y. K. (2000). Effect of self-efficacy conditions of mutual-aid organization members. Social Behavior and Personality: An international journal, 28 (5), 413-422.
Clarke, D. E. (1995). Vulnerability to stress as a function of age, sex, locus of control, hardiness and type A personality. Social Behavior and Personality: An international journal, 23 (3), 285-286.
Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24, 385-396.
Cohen, S., Kessler, R. C., & Gordon, L. U. (1995). Strategies for measuring stress in studies of psychiatric and physical disorders. In S. Cohen, R. C. Kessler, & L. U. Gordon (Eds.), Measuring stress: A guide for health and social scientists (pp. 80-101). New York: Oxford University Press.
Cohen, S., & Williamson, G. (1988). Perceived stress in a probability sample of the United States. In S. Spacapan & S. Oskamp (Eds.), The social psychology of health (pp. 31-67). Newbury Park, CA: Sage.
Dougall, A. L., & Baum, A. (2001). Stress, health and illness. In A. Baum, T. A. Reversion, & J. E. Singer (Eds.), Handbook of health psychology (pp. 321-337). Mahwah, NJ: Lawrence Erlbaum.
Endler, N. S., Kocovski, N. L., & Macrodimitris, S. D. (2001). Coping, efficacy, and perceived control in acute versus chronic illness. Personal and Individual Differences, 30, 617-625.
Figueria-McDonough, J. (1998). Voices of young people in poor inner-city neighborhoods. Youth and Society, 30, 123-163.
Goldberg, D. P., & Hillier, V. (1979). A scaled version of the General Health Questionnaire. Psychological Medicine, 9, 139-145.
Goldberg, D. P., & Williams, P. A. (1988). A user’s guide to the General Health Questionnaire. Berkshire, England: NFER-Nelson.
Islamic Republic of Iran, Ministry of Health and Medical Education (IRIMHME). (2000). Iran demographic and health survey /DHS-2000, p.9.
Keeney, G. B., Cassata, L., & McElmury, B. J. (2004). Adolescent health and development in nursing and midwifery education. Retrieved November 25, 2005, from http://www.who.int/child-adolescent-health/New-publication/aDH/WHO-FCH-CaH.
Kendall, P. C. (1994). Treating anxiety disorders in children: Results of a randomized clinical trial. Journal of Consulting and Clinical Psychology, 62, 100-110.
Kiecolt-Glaser, J. K., McGuire, L., Robles, T. F., & Glaser, R. (2002). Psychoneuroimmunology: Psychological influences on immune function and health. Journal of Consulting and Clinical Psychology, 70, 537-547.
Lewinsohn, P. M., Clarke, G. N., Hops, H., & Andrews, J. (1990). Cognitive-behavioral group treatment of depression in adolescents. Behavior Therapy, 21, 385-401.
Maciejewski, P. K., Prigerson, H. G., & Mazure, C. M. (2000). Self-efficacy as a moderator between stressful life events and depressive symptoms: Differences based on history of prior depression. British Journal of Psychiatry, 176, 373-378.
Monk, E. M. (2004). Student mental health: The case studies. Counseling Psychology Quarterly, 17 (4), 395-412.
Muris, P. (2002). Relationships between self-efficacy and symptom of anxiety disorders and depression in a normal adolescent sample. Personality and Individual Differences, 32 (2), 337- 348.
Muris, P., Schmidt, H., Lambrichs, R., & Meesters, C. (2001). Protective and vulnerability factors of depression in normal adolescents. Behavior Research and Therapy, 39 (5), 555-565.
Nezami, E., Schwarzer, R., & Jerusalem, M. (1996). Persian adaptation of the General Self-Efficacy Scale. Retrieved on November 15, 2004, from http://www.userpage.Fu-berlin.De/health /Persian. html
Pakenham, K. I. (1999). Adjustment to multiple sclerosis: Application of a stress and coping model. Health Psychology, 18, 383-392.
Rawson, H. E., Bloomer, K., & Kendall, A. (1994). Stress, anxiety, depression and physical illness in college students. Journal of Genetic Psychology, 155 (3), 321-33.
Schiaffino, K. M., & Revenson, T. A. (1992). The role of perceived self-efficacy, perceived control and causal attributions in adaptation to rheumatoid arthritis: Distinguishing mediator from moderator effects. Personality and Social Psychology Bulletin, 18, 709-718.
Schwarzer, R., & Jerusalem, M. (1995). Generalized Self-efficacy Scale. In J. Weinman, S. Wright, & M. Johnston (Eds.), Measures in health psychology: A user’s portfolio. Causal and control beliefs (pp. 35-37). Windsor, UK: NFER-Nelson.
Selye, H. (1956). The stress of life. New York: McGraw-Hill.
Shelley, M., & Pakenham, K. I. (2004). External health locus of control and general self-efficacy: Moderators of emotional distress among university students. Australian Journal of Psychology, 56 (3), 191-199.
Unger, J. B., Li, Y., Johnson, C. A., Gong, J., Chen, X., Li, C. V., Trinidad, D. R., Tran, N. T., & Lo, A. T. (2001). Stressful life events among adolescents in Wuhan, China: Association with smoking, alcohol use and depressive symptoms. International Journal of Behavioral Medicine, 8, 1-18.
Wills, T. A., Sandy, J. M., & Yaeger, A. M. (2002). Stress and smoking in adolescence: A test of directional hypotheses. Health Psychology, 21, 122-130.
Table 1. Descriptive Data for Age, Perceived Stress, General Self-Efficacy and Psychological Well-Being
Table 2. Intercorrelation Among Measures of Perceived Stress, Self-Efficacy and Psychological Well-Being
Notes: (N = 148) *p < 0.05, **p < 0.01
Table 3. Comparing Students with High and Low Levels of Self-Efficacy in Relation to Perceived Stress and Psychological Well-Being
Appreciation is due to reviewers including
Sarah O. Meadows
PhD
Center for Research on Child Well-being
Office of Population Research
Princeton University
286 Wallace Hall
Princeton
NJ 08544-5804
USA
Robert Tait
School of Psychiatry and Clinical Neurosciences
University of Western Australia (MPC 521)
QE II Medical Centre
Nedlands
WA 6907
Australia